
“Marley was dead: to begin with. There is no doubt whatever about that.” [A Christmas Carol, Charles Dickens, 1843]
“Is care.data dead?” I was asked after our children’s nativity today, “what happened to that GP record sharing project?” The local priest, you may think of all people, wondered what had become of the news stories we had discussed at Easter.
Not dead, I assured him, though it was suggested recently that the Caldicott led Independent Information Governance Oversight Panel (IIGOP) report [1], would be the final nail in the coffin of the past approach [2], and would spell doom ahead in any care.data future were the programme not to follow its recommendations.
I told him the story of the care.data year.
So, are you sitting comfortably? For Christmas is a time of storytelling. At its heart, the story of a birth, which has been handed down through generations.
But here, I borrow from the most famous of all English Christmas stories, a Christmas Carol, by Charles Dickens from 1843. Let us begin.
“Come in!” exclaimed the Ghost. “Come in! and know me better, man!”
The ghost of care.data past rattled its chains and brought no joy in 2014, haunting the current programme with news of past data sharing practices. At the start of the year, much was made of the 25 years of past use of our health records with third parties about which the public had never been told nor asked for permission, we were told there had never been breaches [3], and there was surprise expressed by NHS England leadership at why care.data, the plan to extract GP records now in addition, should have struck such a nerve in the public. Then they actually ran an audit that told the full story.
Various reports have since tried to vanquish those ghosts which have haunted the rollout of care.data in the past year. Sir Nick Partridge in May led the Review of Data Releases by the NHS IC which looked back at health data sharing of the existing HSCIC held data, and in November, he examined the progress up to the present.[4] The extent of third party releases including actuarial firms, organisations in the US and China, and commercial re-use was a complete surprise to the public and, his report appeared to suggest to many like him in management as well.
The IIGOP Report published last week on the care.data Programme Board looks to the future. It sets out a thorough set of specific recommendations, questions and tests to meet before it could be reasonable to proceed to a data extraction in the care.data pilot.
The first independent report on care.data, prepared and released under the oversight of the new Data Guardian, Dame Fiona Caldicott, it also captures many sensible and practical questions raised by patients at events all year.
In some ways, whilst sad to see what so many have said was needed has only come to be addressed by an independent body rather than NHS England, recognising the current weaknesses can only be seen as positive to bring about changes. It may have a hope of restoring public and professional trust.
What next steps will come from this for a care.data relaunch by NHS England, and when in future, remain to be seen. [Updates may be here, or here or sometimes here].
Perhaps if the current course of actions is averted, we may not ‘see a vacant seat’ if it all falls apart in 2015 after all.
The CCGs have been given a huge responsibility which is not of their making, if NHS England continues to pilot under CCG-steered rollouts.[5]
One would hope that given the right amount of time needed to manage this change process, and with the right supporting skills and tools for the practicalities, the care.data programme will take a changed form in the year ahead. It may yet be saved.
But it does seem often that timing is of the essence, and we move from one artificial deadline to the next. The public and GPs wait without the security and confidence of a realistic schedule. Waiting we wonder if we will reach the next chime due, or the next ghost to haunt the programme will arrive and cause new fright.
It’s no cure all, but it appears the IIGOP has given the programme the gift of one last wonderful opportunity to get this right. It’s requirements are sizeable and will take time to execute sensibly. The report illuminates a future path for progress and shows what must be altered today, to avoid the future it predicts otherwise.
The outcome of care.data rests in the hands of the DH and NHS England. Dependent on the public and professions seeing change.
As Scrooge learns:
“But if the courses be departed from, the ends will change.” [A Christmas Carol, Charles Dickens, 1843]
Ignore the wisdom of the ghosts at your peril. For a changed future outcome, the actions of the present must change first.
So, humour me awhile, and let’s consider some of the bigger themes in the care.data Christmas carol that CCGs may wish to consider as it deals with preparing for pathfinder pilots…
Chapter 1. “This boy is Ignorance. This girl is Want. Beware them both, and all of their degree, but most of all beware this boy, for on his brow I see that written which is Doom, unless the writing be erased…” [A Christmas Carol, Charles Dickens, 1843]”
What information is getting through from listening events? [6]
There should be no excuse for poverty in the world today, and whilst in my bigger picture wish list, to deal with want would come first, in my care.data Christmas carol list, it is ignorance which cannot be tolerated.
There is no excuse for ignorance, for lack of information, or wondering what questions needed answers to date at the care.data programme board of NHS England.
“How do we explain care.data vs SCR”, “Can you tell me exactly who will access my data?”, “If future purposes change and I want the opportunity to withdraw & opt out, how will I get told?”
The IIGOP report states clearly the current gaps in knowledge and what must be done to fill them, for various parties.
Together with two other major reports this year on health data sharing and care.data: Partridge, and the November 2014 APPG report [7], professional bodies have provided plenty of information and asked plenty of questions which no one now can ignore.
Misplaced statements that there have been no breaches do nothing for public confidence, when later reports show that is ignorant or inaccurate. Big Brother Watch published its report into NHS Data Breaches in November. It found that data security is an ongoing problem, and that over the last four years patient confidentiality had been breached at least 7,255 times.[8]
Facts and answers now need to address the IIGOP report in depth, and meet patients’ past questions, to lay to rest some of the issues which have haunted the programme in the press; unexpected commercial uses, and re-use of data through commercial data licenses, for example.
Adequate time must be given to the CCGs, GPs and patients to be fully informed of the programme and the choice(s) on offer. This is not an IT rollout, but a series of process changes, which need human understanding and acceptance. “What’s in it for me?” versus “What risks may harm me?” need thinking time to be fairly presented and the patient choice collected.
To avoid potential doom whether it be significant opt out or failure to meet fair processing leaving GPs at risk [9], to adequately communicate through effective education, will take effort.
Chapter 2. “Every one of them wore chains like Marley’s Ghost; some few (they might be guilty governments) were linked together; none were free.” [A Christmas Carol, Charles Dickens, 1843]
Understand the links of who, why and what, of data sharing:
The decision making, the process steps, how patients are told of changes in the programme today and will be in future, how the public perceives their data is exploited, are all linked together by very simply: who stores and uses the data, and for what purposes.
For the programme, it would be wise to understand the importance of the interaction of these parts of the process. Linked appropriately together, and working well, trust will keep the system together. It fails, and no matter how good the technology is, without trust, the system will fail to deliver its expectations. If too many may opt out, or opt out disproportionately in certain population segments it would harm data quality.
When at the HSCIC data sharing discussion in July it was clear some data recipients were yet to grasp this interdependency, and the effect their attitudes to data use have on each other.
If one [class of] data recipient in future receives or uses data inappropriately, it will harm public faith in all users.
For patients, to have true transparency I believe care.data should be explaining exactly how the data linkage system [10] works, and all the other silos of data it already holds. The personal demographics service, stores a whole set of personal data of which the public maybe unaware, and yet may find used to link data collected from all sorts of parts of health and social care. If NHS data sharing is to be explained, do it all. To avoid doing this, will merely store up a future risk of yet more surprises for patients and damage trust further.
Chapter 3: “I have seen your nobler aspirations fall off one by one, until the master-passion, Gain, engrosses you.” [A Christmas Carol, Charles Dickens, 1843]
Commercial use of data will be detrimental to public confidence.
By looking ahead to see what the ghost of care.data future might bring, the forecast doom of the present course, may yet be avoided.
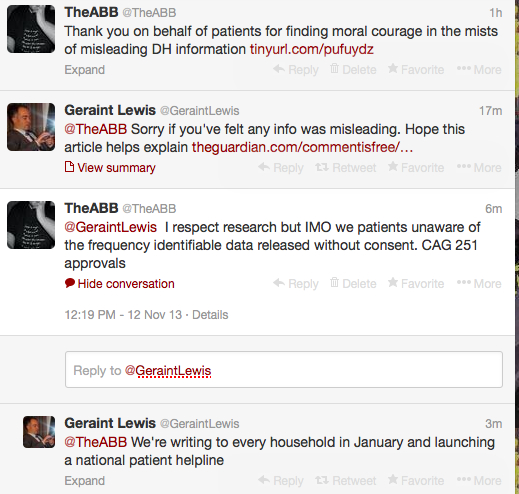
As patients told NHS England at the Open House event [11], we’re fed up with commercial data mining, and the same was reflected by a representative group of citizens in various polls this year.[12]
How is the non-NHS data world changing? What of the upcoming EU data legislation? How does commercial data industry itself perceive legislation in the UK?
In the 2013 Experian keynote address the Nectar Head of Customer Marketing noted, “legislation has not kept up to speed with where we are going’ [16:57] [13]
Perhaps it is opportune to reflect on one of the oldest Biblical themes at Christmas, choose which master you serve.
Back at NHS England and the IC, discussions in April 2013 seek to ‘create a vibrant market of data intermediaries , for example.
Which purposes should this serve? The health of the nation, or the wealth of the nation? Can one justly serve both equally?
“You fear the world too much,” she answered, gently. “All your other hopes have merged into the hope of being beyond the chance of its sordid reproach. I have seen your nobler aspirations fall off one by one, until the master-passion, Gain, engrosses you.” [A Christmas Carol, Charles Dickens, 1843]
It would appear to patients that by mixing commercial purposes in with legitimate health, and health research purposes, the data commissioning system has created its own downfall.[14]
The purposes whilst amended in the Care Act 2014, are so broad as to leave too much commercial use open under ‘purposes of health’. How would that rule out pharmaceutical marketing for example?
For many patients, use outside their own healthcare and its provision and planning is a real hot chestnut.
If patients are in disagreement over commercial uses for example, they have no choice but to opt out of research uses as well. This multi-option choice, or the removal of commercial use needs addressed.
If research wants more data, we would do well to define and restrict commercial use in legislation, much more specifically.
Chapter 4 : “You wish to be anonymous?” [a Christmas Carol, 1843]
There has been much disagreement and misunderstanding of how data will be used, anonymous or what non-identifiable really means.
Media reporting at the start of the year frequently focused on the collection of care.data as ‘anonymous data.’ Bah, humbug! that is factually incorrect.
CCGs need to make sure that their own staff understanding is correct, as well as passing on information if they are to be intermediaries on behalf of NHS England. At CCG meetings I attended, many staff confused care.data with direct care/SCR.
The default position if patients do nothing is the sharing of date of birth, full postcode, gender and ethnicity, and the NHS number is a unique identifier. Plus all the other codes and conditions.
It is still unclear how the data which has already been extracted without consent or fair processing, can be controlled by patients who may not wish to share identifiable data from their hospital visits, mental or community health.

If patients can’t control data already held at HSCIC, why will they want to share more additional data, from primary care?
Learning from looking back on 2014
My own looking back on my care.data journey in 2014 is here.
medConfidential has a rather good summary of the year here. [15]
“Spirit,” said Scrooge submissively, “conduct me where you will. I went forth last night on compulsion, and I learnt a lesson which is working now. To-night, if you have aught to teach me, let me profit by it.” [A Christmas Carol, Charles Dickens, 1843]
From past lessons learned in 2014, one would hope the future rollout will profit from them and take the time, and use the tools it needs, to get to a brighter future.
Looking ahead: news for 2015 came at the end of the year.
Sir Partridge in the Telegraph, November 27 he said:
“We must make sure there are no surprises for the public about how their information is being used, that they have a choice in this and that we are honest about the balance of risk. Every single one of us has a part to play in making sure we get this right…
“The HSCIC is still improving its practices. It is also endeavouring to increase its transparency.”
“the public had been inadequately consulted in the early stages of the Care.data programme and that it was therefore correct to halt the programme to allow further public consultation.” [APPG report]
It goes on to say, “Organisations providing health or social care services must succeed in both respects [examining the Public Interest] if they are not to fail the people that they exist to serve,” and with that in mind a Public Benefits Plan should be drawn up, to support public transparency.
Public transparency would be improved by publishing the public’s questions from multiple listening events at which attendees were promised answers and follow up. The conversations did not always ask easy questions, but all the more reason to address them publicly for all; it will make the programme better.
So, if the care.data programme learns from that which has haunted care.data in the past year, and NHS England now grapples with all the questions and criteria of the IIGOP report, and increases its public transparency, stakeholders can look to the future with a renewed hope. But only if there is change made to the present course of actions.
“Scrooge was at first inclined to be surprised that the Spirit should attach importance to conversations apparently so trivial; feeling assured that they must have some hidden purpose.” [A Christmas Carol]
“What do you think of the show so far?”
Clearly the National Data Guardian and IIGOP, the APPG and others making many wise recommendations, find the approach so far lacking. To carry on as is, will bring predictable doom. But by using the IIGOP report insights, there is the hope that the outcomes of the current path may yet be avoided.
Which version of the care.data future will the NHS England Patients and Information Directorate choose to follow, and invite the CCGs to join them on, writing the next chapter of the care.data story in 2015?
“No space of regret can make amends for one life’s opportunity misused.” [A Christmas Carol, Charles Dickens, 1843]
***
Let’s hope 2015 is a good year, that the wish list of questions finds answers, and let’s hope there are no more care.data surprises.
“I HAVE endeavoured in this Ghostly little book, to raise the Ghost of an Idea, which shall not put my readers out of humour with themselves, with each other, with the season, or with me. May it haunt their houses pleasantly, and no one wish to lay it.
Their faithful Friend and Servant,
C. D.“
“What’s to-day, my fine fellow?” said Scrooge.
“To-day!” replied the boy. “Why, Christmas Day.”
“Merry Christmas, and so, as Tiny Tim observed, God bless Us, Every One!”
***
Image from a Muppets Christmas Carol, 1992
References:
[1] The IIGOP report https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/389219/IIGOP_care.data.pdf
[2] EHI ‘Care.data Review Raises Questions‘ http://www.ehi.co.uk/news/ehi/9808/care.data-review-raises-questions
[3] BBC Radio 4, February 4 2014 http://www.bbc.co.uk/programmes/p01rmpdy
[4] Nov 2014, Progress of HSCIC data sharing review by Sir Nick Partridge https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/380042/HSCIC_Report_Summary_of_progress_261114_FINAL.pdf
[5] 7 Oct 2014, CCGs to help deliver care.data pilots http://www.england.nhs.uk/2014/10/07/ccgs-care-data-programme/
[6] What information is being heard at Listening events? https://jenpersson.com/pathfinder/
[7]The APPG Report – Nov 2014 – http://www.patients-association.com/Portals/0/APPG%20Report%20on%20Care%20data.pdf
[8] Report into NHS Data breaches http://www.bigbrotherwatch.org.uk/wp-content/uploads/2014/11/EMBARGO-0001-FRIDAY-14-NOVEMBER-BBW-NHS-Data-Breaches-Report.pdf
[9] on GP indemnity: care.data MPS advice to members http://www.medicalprotection.org/uk/membership-indemnity-updates/care.data
[10] The data linkage service http://www.hscic.gov.uk/media/12443/data-linkage-service-charges-2013-2014-updated/pdf/dles_service_charges__2013_14_V10_050913.pdf
[11] The Open House June 2014, public questions https://jenpersson.com/care-data-communications-core-concepts-part-two/
[12] Privacy and Personal Data IPSOS Mori poll https://www.ipsos-mori.com/researchpublications/researcharchive/3407/Privacy-and-personal-data.aspx
[13] 2013 Experian keynote address the Nectar Head of Customer Marketing
[14] care.data downfall parody http://paulbernal.wordpress.com/2014/02/25/tim-kelsey-discovers-care-data-is-in-trouble/
[15] medConfidential bulletin https://medconfidential.org/2014/medconfidential-bulletin-19-december-2014/

![Launching genomics, lifeboats, & care.data [part 2]](https://jenpersson.com/wp-content/uploads/2014/08/rosetta_image-672x372.jpg)

{kind=link}