![Building Public Trust in care.data sharing [1]: Seven step summary to a new approach](https://jenpersson.com/wp-content/uploads/2015/07/edison1-672x372.jpg)
Here’s my opinion after taking part in the NIB #health2020 Bristol event 24/7/2015 and presentation of plans at the June King’s Fund hosted event. Data sharing includes plans for extraction and uses of primary care data by third parties, charging ahead under the care.data banner.
Wearing my hat from a previous role in change management and communications, I share my thoughts in the hope the current approach can adapt and benefit from outside perspectives.
The aim of “Rebuilding and sustaining Public trust” [1] needs refocused to treat the cause, not only the symptoms of the damage done in 2014. Here’s why:
A Seven Step Top Line Summary
1. Abstract ‘public trust’ is not vital to the future of data sharing. Being demonstrably worthy of public trust is.
2. Data-sharing is not vital to future-proof the NHS. Using knowledge wisely is.
3. A timed target to ‘get the public’s data’, is not what is needed. Having a stable, long term future-proofed and governable model is.
4. Tech solutions do not create trust. Enable the positive human response to what the org wants from people, enabling their confident ‘yes to data-sharing.’ [It might be supported by technology-based tools.]
5. Communications that tell the public ‘we know best, trust us’ fail. While professional bodies [BMA [2], GPES advisory group, APPG report calling for a public benefits plan, ICO, and expert advice such as Caldicott] are ignored or remain to be acted upon, it remains challenging for the public to see how the programme’s needs, motives and methods are trustworthy. “The [Caldicott 2] Review Panel found that commissioners do not need dispensation from confidentiality, human rights & data protection law.” [3] Something’s gotta give. What will it be?
6. care.data consistency. Relationships must be reliable and have integrity.
“Trust us – see the benefits” [But we won’t share the business cost/benefit plan.]
“Trust us – we’re transparent” [But there is nothing published in 2015 at all from the programme board minutes] [4]
“Trust us – we’ll only use your data wisely, with the patient in control” [Ignore that we didn’t before [5] and that we still share your data for secondary uses even if you opted out [6] and no, we can’t tell you when it will be fixed…]
7. Voices do not exist in a vacuum. Being trustworthy on care.data does not stand alone but is part of the NHS ‘big picture’.
Department of Health to GPs: “Trust us about data sharing.’ [And ignore that we haven’t respected many of your judgement or opinions.]
NHS England to GPs: “Trust us about data sharing.’ [And ignore our lack of general GP support: MPIG withdrawal, misrepresentation in CQC reports] NHS England and Department of Health to professionals and public: “The NHS is safe in our hands.’ Everyone: “We see no evidence that plans for cost savings, 7 day working, closures and the 5YFV integration will bring the promised benefits. Let us ‘see the holes’, so that we can trust you based on evidence.”
See the differences?
Target the cause not Symptom:
The focus in the first half, the language used by NHS England/NIB/ DH, sets out their expectations of the public. “You must trust us and how you give us your data.”
The focus should instead to be on the second half, a shift to the organisation, the NHS England/NIB/ DH, and set out expectations from the public point-of-view. ” Enable the public to trust the organisation. Enable individual citizens to trust what is said by individual leaders. This will enable citizens to be consensual sharers in the activity your organisation imposes – the demand for care.data through a statutory gateway, obliging GPs to disclose patient data.
The fact that trust is broken, and specifically to data-sharing that there is the deficit [A] between how much the public trusts the organisation and how the organisation handles data, is not the fault of the public, or “1.4 M NHS staff”, or the media, or patient groups’ pressure. It’s based on proven experience.
It’s based on how organisations have handled data in the past. [5] Specifically on the decisions made by DH, and the Information Centre and leaders in between. Those who chose to sell patient data without asking the public.
The fact that trust is broken is based on how leadership individuals in those organisations have responded to that. Often taking no responsibility for loss.
No matter how often we hear “commissioners will get a better joined up picture of care needs and benefit you”, it does not compensate for past failings.
Only demonstrable actions to show why it will not happen in future can start that healing process.
Target the timing to the solution, not a shipping deadline
“Building trust to enable data sharing” aims at quick fixes, when what is needed is a healing process and ongoing relationship maintenance.
Timing has to be tailored to what needs done, not an ‘artificial deadline’. Despite that being said it doesn’t seem to match reality.
Addressing the Symptoms and not the Cause, will not find a Cure
What needs done?
Lack of public trust, the data trust deficit [A] are symptoms in the public to be understood. But it is the causes in the organisations that must be treated.
So far many NHS England staff I have met in relation to care.data, appear to have a “them and us” mentality. It’s almost tangibly wrapped up in the language used at these meetings or in defensive derision of public concerns: “Tin foil hat wearers”, “Luddites” [7] and my personal favourite, ‘Consent fetishists.’ [8] It’s counter productive and seems borne from either a lack of understanding, or frustration.
The NIB/DH/NHS England/ P&I Directorate must accept they cannot force any consensual change in an emotion-based belief based on past experiences, held by the public.
Those people each have different starting points of knowledge and beliefs. As one attendee said, “There is no single patient replicated 60 million times.”
The NIB/DH/NHS England/ P&I Directorate can only change what they themselves can control. They have to model and be seen to model change that is trustworthy.
How can an organisation demonstrate it is trustworthy?
This means shifting the focus of the responsibility for change from public and professionals, to leadership organisation.
There is a start in this work stream, but there is little new that is concrete.
The National Data Guardian (NDG) role has been going to be put on a legal footing “at the earliest opportunity” since November 2014. [9] Nine months.
Updated information governance guidance is on the way.
Then there’s two really strong new items that would underpin public trust, to be planned in a ‘roadmap’: the first a system that can record and share consent decisions and the second, to provide information on the use to which an individual’s data has been put.
How and when those two keystones to public trust will be actually offered appear unknown. They will encourage public trust by enabling choice and control of our data. So I would ask, if we’re not there yet on the roadmap, how can consent options be explained to the public in care.data communications, if there is as yet no mechanism to record and effect them? More on that later.
Secondly, when will a usage report be available? That will be the proof to demonstrate that what was offered, was honoured. It is one of the few tools the organisation(s) can offer to demonstrate they are trustworthy: you said, we did. So again, why jeopardise public trust by rolling out data extractions into the existing, less trustworthy environment?
How well this is done will determine whether it can realise its hoped for benefits. How the driving leadership influences that outcome, will be about the organisational approach to opt out, communicating care.data content decisions, the way and the channels in which they are communicated, accepting what has not worked to date and planning long-term approaches to communicating change before you start the pathfinders. [Detailed steps on this follows.]
Considering the programme’s importance we have been told, it’s vital to get right. [10]
i believe changing the approach from explaining benefits and focus on public trust, to demonstrating why the public should trust demonstrable changes made, will make all the difference.
So before rolling out next data sharing steps think hard what the possible benefits and risks will be, versus waiting for a better environment to do it in.
Conclusion: Trust is not about the public. Public trust is about the organisation being trustworthy. Over to you, orgs.
####
To follow, for those interested in nitty gritty, some practical suggestions for progress in Building Public Trust in data sharing:
This is Part one: A seven step top line summary – What I’d like to see change addressing public trust in health data sharing for secondary purposes.
Part two: a New Approach is needed to understanding Public Trust For those interested in a detailed approach on Trust. What Practical and Policy steps influence trust. On Research and Commissioning. Trust is not homogeneous. Trust is nuanced even within the single relationship between one individual and another. It doesn’t exist in a vacuum.
Part three: Know where you’re starting from. What behaviours influence trust. Fixing what has already been communicated is vital before new communications get rolled out. Vital to content of your communications and vital for public trust and credibility.
Part four: Communicate the Benefits won’t work – How Communications influence trust. For those interested in more in-depth reasons, I outline in part two why the communications approach is not working, why the focus on ‘benefits’ is wrong, and fixes.
Part five: Future solutions – why a new approach may work better for future trust – not to attempt to rebuild trust where there is now none, but strengthen what is already trusted and fix today’s flawed behaviours; honesty and reliability, that are vital to future proofing trust
####
Background References:
I’m passionate about people using technology to make their jobs and lives better, simpler, and about living well. So much so, that this became over 5000 words. To solve that, I’ve assumed a baseline knowledge and I will follow up with separate posts on why a new approach is needed to understanding “Public Trust”, to “Communicating the benefits” and “Being trustworthy and other future solutions”.
If this is all new, welcome, and I suggest you look over some of the past 18 months posts that include public voice captured from eight care.data events in 2014. care.data is about data sharing for secondary purposes not direct care.
[1] NHS England October 2014 http://www.england.nhs.uk/2014/10/23/nhs-leaders-vision/
[2] BMA LMC Vote 2014 http://bma.org.uk/news-views-analysis/news/2014/june/patients-medical-data-sacrosanct-declares–bma
[3] Caldicott Review 2: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/192572/2900774_InfoGovernance_accv2.pdf
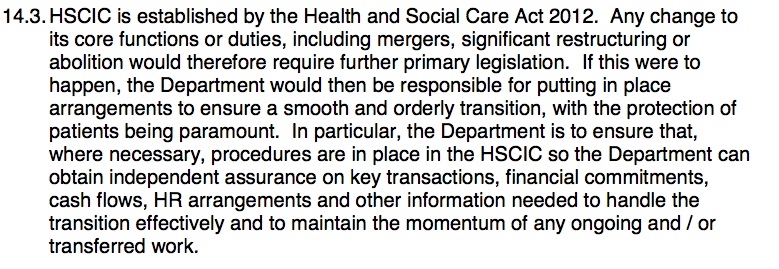
[4] Missing Programme Board documents: 2015 and June-October 2014
[5] HSCIC Data release register
[6] Telegraph article on Type 2 opt out http://www.telegraph.co.uk/news/health/news/11655777/Nearly-1million-patients-could-be-having-confidential-data-shared-against-their-wishes.html
[7] Why Wanting a Better Care.Data is not Luddite: http://davidg-flatout.blogspot.co.uk/2014/04/why-wanting-better-caredata-is-not.html
[8] Talking to the public about using their data is crucial- David Walker, StatsLife http://www.statslife.org.uk/opinion/1316-talking-to-the-public-about-using-their-data-is-crucial
[9] Dame Fiona Caldicott appointed in new role as National Data Guardian
[10] Without care.data health service has no future says director http://www.computerweekly.com/news/2240216402/Without-Caredata-we-wont-have-a-health-service-for-much-longer-says-NHS
Polls of public feeling:
[A] Royal Statistical Society Data Trust Deficit http://www.statslife.org.uk/news/1672-new-rss-research-finds-data-trust-deficit-with-lessons-for-policymakers
(B] Dialogue on data – work carried out through the ADRN

![The Economic Value of Data vs the Public Good? [3] The value of public voice.](https://jenpersson.com/wp-content/uploads/2015/03/Trust-e1426443553441-672x372.jpg)