“My concerns about care.data are heightened, not allayed by the NHS England apparently relentless roll-out and focus on communications. Whilst they say it will take as long as it needs, there is talk of Oct-Nov. pilots. It is still all about finding the right communications, not fixing flaws in core concepts.”
For part one of this post see here >>care.data communications and core concepts [Part one]
 Other sessions on the 17th Open House included:
Other sessions on the 17th Open House included:
Patient participation in general practice: exploring how can you be involved in the changes in general practice, including the introduction of the Friends and Family Test and changes to the GP contract in relation to Patient Participation Groups.
Patients Online: This session was to enable attendees to find out more about work to increase the number of patients who can access their health records online, book GP appointments online and order repeat prescriptions. The accompanying film was described by a fellow table guest as, ‘awful. Too long, dull and dry.’ It felt that there was a lot of weight given to this part of the day and that the uses of data during the event were all mixed into one pot. care.data will not be the source for patient online access, yet we came away thinking of the data as one source to enable that purpose. Poor communication or clever marketing, will depend on your point of view.
The big picture however, of how our health records will be used and bring benefit is in my opinion, being manipulated and purposes conflated to make one thing seemingly lead to another, which are in fact unrelated.
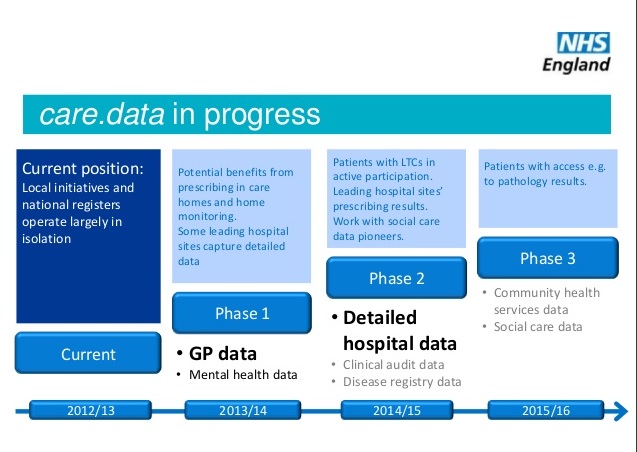
care.data is for secondary purposes, not direct care use by physicians for example. We are told this sharing of data is a requirement for other things as well. Firstly for patient safety and quality. And for integration between services.
Integration
Mr.Kelsey said at the Open House day, (around 36:00 minutes in, if you listen yourself) “we’ve all heard this word integration, I’m not terribly sure what it means, but I think what it means is that local people have a proper say in the way that health services are designed. So to give you voice, to give the local community voice, care.data is really important….”
I should hope that Mr.Kelsey has a jolly good understanding of integration and knows exactly that it is the merging of health and social care under the motto ‘transformation’. Social care under ADASS and health care are under all sorts of pressures to integrate, budgets are being pooled, shared and ring-fenced in various discussions, including my local county Health & Adult Social Care Select Committee:
“…Director Adults’ Services, told the (Chichester) Committee [9] in November 2013: The Care Bill would mean a radical whole system change involving the biggest ever transformational change for Adults’ Services The Council was building the foundations for further significant change.”
Mr. Kelsey did, in his speech note however, that the programme should be respecting the fact it is *their* data, *not* the NHSs. (This is in contrast to his previous position in which patients should not be given an opt out choice – Prospect Magazine, 2009 when his stance was “no one who uses a public service should be allowed to opt out of sharing their records. Nor can people rely on their record being anonymised”).
It’s an argument oft repeated that we should *own* our data, but somewhat meaningless if it took a campaign and public outcry to require an opt out mechanism, and put the programme on hold. I feel the language is being manipulated to create the impression we don’t already own or have rights to our health data. The opposite is true. And many know that, just see the killer question below from Leicester. As long as records are held only at GP level, we will have much greater control and visibility of their use, than if shared centrally.
Many I have spoken with ask why it is not possible to leave data at local GP level for only clinical care, and extract nothing identifiable from hospitals without consent?
Other People’s Questions
In that vein, I summarise what 4 other people asked Mr. Kelsey and his panel in London about care.data on the day, and what I felt was missing from the answers to give balanced communications. The locations of about 80-100 people at each, were each allowed to put forward one question to the panel via web link, the question selected from all those discussed at the tables, by an organiser at the site. They covered Benefits / Data Uses / Confidentiality / Communications.
View them for yourself here, from 01:13.06 in the NHS Open House video:
Question selected to be asked from Basingstoke: “If people opt out of giving data will then the results not then be inaccurate?”
The larger volume of data, the better quality the data will be, the greater the benefits will be. Choosing not to opt out. That will, depending on the volume of that, affect data quality to a degree we won’t know that. Over time, once people’s concerns have been addressed, we hope that quality will improve.
Missing from the answer: [10] HES data is cleaned, SUS data is not, and both are known to have significant quality issues on validity and accuracy. The data has been extracted and stored for twenty plus years. Higher volume of data does not equate with a higher quality of data. You don’t make a better quality haystack, just by adding more hay. The volume of data is less important than it be representative of all parts of the population, but there is a risk that those opting out tend to be, as one GP has told me, ‘the white middle class and educated leaving others overly represented’. Only having more data is not a solution for quality.
*****
Question from Leicester: “Are we saying there will be only clinical use of the data – no marketing, no insurance, no profit making? This is our data.”
Panel: New legislation was brought in which made it very clear, data could only be released for the benefit for health and care, and it cannot be released solely for commercial purposes – yes, data can go to a private sector organisation, yes commercial companies, but only where they are working for the benefit of health and care, for example, Dr.Foster Intelligence, or other data information intermediaries who do a lot of work with data and who do a lot of work with the NHS to help inform decisions. Data will still be available to commercial companies. The other point, there is going to be independent scrutiny, which will be formalised within the law, to have independent scrutiny by the Confidentiality Advisory Group, which already exists which can independently scrutinise the releases.
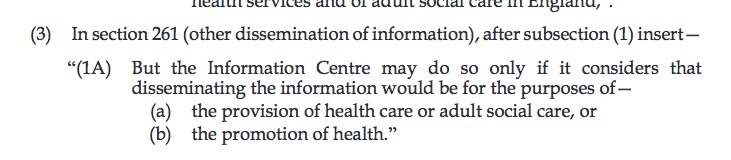
Missing from the answer: care.data is not for clinical care. This indeed is our data and belongs to patients not NHS England, and should be respected as the NHS Constitution requires. Data continues to be released, and will continue to be so even under the Care Act legislation, to third parties in financial transactions. No recipient organisation by function (such as insurance) is excluded per se, rather recipients are judged based on their intended use of the data. The precise terms are open under the Act :
 ****
****
Question from London: “How do you propose to reset expectations and perceptions, with any future communications, and given that the way the first round was handled, provoked apparently such strong public resistance and suspicion about the NHS England motives?”
Panel spokesperson: We didn’t get it right the first time round, partly because we approached that at the National level. There was a leaflet that went out nationally. We will work with the 100-500 GP practices, and work co-produce materials in those areas and work with what is already there locally, GP practices, LMCs, PPGS, Healthwatch, using local knowledge, and patients so we can make sure everyone can understand, we understand how we can communicate this, what the concerns are, so we can get the message across, so everyone can understand what the choice is and what this is about.
Mr.Kelsey added: …[…]This isn’t about us and you, this is about us collectively. How do we ask patients and citizens for permission to use their personal information…we need to get that conversation right.”
Communications materials
Draft FAQs and information sheets to use in those conversations were on the table for participants information and to take away. The Data Uses page wording is interesting but poorly phrased, as it misled a couple on my table to think the ‘extraction’ was not identifiable. (see point 9 above). And the Benefits case study header is “How might it reduce variations in cancer treatment & care” but concludes that actually the Cancer Registry already does this, and they instead mean something similar would be useful for diabetes. This misuse of benefits makes me think, they’re finding it jolly difficult to find real ones. But if we all at these public meetings, believe the presented stories with the positive spin as fact, then fact they will become.
“And if all others accepted the lie which the Party imposed—if all records told the same tale—then the lie passed into history and became truth.” (George Orwell, 1984)
What next?
It is vital in my mind that care.data communications match reality of what needs done technically and in procedures, to drive expectations of what care.data will deliver and when. Why does an easy read brochure make no mention whatever of who data may be sold to? There is no mention of what organisations continue to receive HES and wider data. Instead it talks about data being shared to ‘know the health needs of everyone’ yet the very people who are outside the system are the ones whose needs we don’t know today – there is a huge amount known from the rest of the existing patients’ needs from QOF and other GP data extractions, even that used in CPRD for research – purposes for which GP records under care.data are not approved.
The current doublespeak between the comms message and the reality are so far apart, between the technical possibility of what can be done well now, and what needs done to achieve the hoped for benefits, that the current message is setting up the project for failure and benefits will not be realised any time soon. It’s not ready to roll out through ‘improved communications’.
To be fair, the smaller workshop I attended on the 27th, flagged ‘still need to consider how best to engage here’ with many population groups. But it appears to me the Communications teams are effectively doing their best to package something which is not ready to be wrapped. To dot the i on the report, when the chapters aren’t in place yet.
“They were engaged in producing something called an Interim Report, but what it was that they were reporting on he had never definitely found out. It was something to do with the question of whether commas should be placed inside brackets, or outside..” [1984, George Orwell]
I’ve worked on both technical and change management/ communications teams [in another industry]. Project teams’ close working and each having an understanding of the other is vital. But the team members I have met so far, appear to work in silos, without enough linkage to know the functional gaps between them, in technical system, procedures and the link to change & comms. There is no way in my lay opinion, that a pilot of these half-formed knowns will be ready for autumn. For the NHS England leadership to continue to plug that it is, with messages of emotional manipulation of why more data is needed, will condemn care.data to Room 101. A tortuous drawn out reformation of an existing concept. When really it needs planned afresh from the ground up to get the needs of the people it should serve designed into its consent, collection and communications processes – not added on as the ribbon at the end.
I was more optimistic about the benefits in the past, as long as the procedures around consent, governance and security were addressed. Having spoken with and listened to the needs and concerns of various charity representatives this week, at another smaller event, I am much less so. Their complex needs, people who go in and out of different parts of the health and social care system at different times in their lives, with real concerns around confidentiality and risks have not begun to be addressed. Real issues for all of disclosure to GPs to ensure care may affect us all. But for many of their clients, they have needs which often carry huge trust and security issues which could put not only their medical care, but their faith in the charities and people working with them, in jeopardy.
“Being in a minority, even in a minority of one, did not make you mad. There was truth and there was untruth, and if you clung to the truth even against the whole world, you were not mad.” (George Orwell, 1984)
I therefore asked the group at the end of the morning workshop, as Mr.Kelsey had done at the Open House event, how many of the attendees were really comfortable and confident that they knew what care.data was so that they could be a go-to point for questions, or even advocate for the programme as NHS England hoped.
Did they understand what data would be extracted, why and used by whom. About 1/6 raised a hand. That’s *after* the event at the end of the morning spent discussing what issues exist for hard-to-reach, or as one attendee said ‘easy-to-ignore’ groups, and how communications channels will reach them.
One said he did not need to know all the facts to help be a comms channel. Another said he wouldn’t advocate for something he himself did not believe in. It was the first time we started to get genuine cross-group discussion, when in the meeting the table model had been employed again, but for those groups, disabilities, challenges, societal issues are not in silos. Real debate, of hard issues is needed, and yes it’s awkward and might not be able to be ‘managed’ in the same way, but it’s real.
Our group identified a similar basic concept need across their client interests – a rolling consent model which allows opt in and out to change over time. Consent not only for what parts of planned uses the data would be used, but should also consider what parts of the record they are happy to share. Military, youth offenders, teens, the at-risk nature of these groups may mean they wish sections of their history to be restricted if not used for clinical care. And they may wish to share data when under the care of a GP but restrict it again, when under a military one. Or teens may be happy to permit data sharing at another time in their lives, but not permit access to their whole history. The DH Youth Offender expert raised the prickly issue of teen confidentiality and how will consent be gathered when parents may not tell them about the scheme at all, thinking there is ‘nothing to know’. We explained the concept of Gillick to the comms staff and that it’s not about an age of consent in the normal legal sense. What happens if a teen finds out their data has been extracted and wants it removed as teen or adult? We asked about name stored in the Personal Demographics Service and asked why data could not be deleted if clinician and patient both agreed a mistake had simply been made.
These complex and simple core questions need asked to get the whole thing built on a sound and trusted foundation. And they need to be in place for a pilot to make it worth having at all.
If the needs, concerns and understanding of the reps in the room can’t be addressed in a dedicated workshop, how will a remote campaign achieve it for the population at large?
Some at our table asked why the system needs more data when you haven’t managed or used much of what we had in the past? I would also ask what progress is to be expected on unresolved quality and procedural issues with the current systems and data? Simply adding more hay to make a bigger haystack, does not make it easier to find a needle.
No wonder we can ask if it is really not just about commercial uses which comms don’t want to talk about, wonder why you never mention the data linkage service using PDS data [5] held and have concerns of overzealous surveillance by Big Brother.
There are risks becoming so heavily reliant on centralised data. Recently, patients have been wrongly deleted from GP lists, leaving them without a doctor through the cleaning firm’s administrative or process error.
Some are concerned that patients lose trust in their GP and withhold information. Others about this honey-pot of data for the individual citizen’s security. Professionals have voiced concern for GPs and consultants if factual misrepresentation by statistics used for ‘ranking and spanking’ will adversely impact their decision making and make them more risk averse. In a negative way. Or with respect to waiting times and treatment, the heavy use of data in measurement creates a risk that it is misrepresenting the facts through lack of context or even, as in several high profile press cases recently, that such pressure is felt, that records are falsified.[12]
“And when memory failed and written records were falsified—when that happened, the claim of the Party to have improved the conditions of human life had got to be accepted, because there did not exist, and never again could exist, any standard against which it could be tested.” (1984, George Orwell)
I’m concerned about all of the above. Perhaps holding care.data in room 101 until it is a manageable and explainable concept, backed up with technically and procedurally sound processes, would be the best place for it, for some time to come. Results and expectations create failure if they cannot marry up in reality. This isn’t about communications. If you don’t really know what you’re communicating and can’t get it understood easily, then it’s back to the drawing board.
My concerns about care.data are heightened, not allayed by the NHS England apparent relentless rollout and focus on communications. Whilst they say in doublespeak it will take as long as it needs, there is talk of a Oct-Nov pilot launch. A pilot must test the finished model at small scale, not a less-than-half-ready one. Whilst the public push is all about finding the right communications, what is needed is fixing flaws in core concepts.
Doing without it, and waiting, would be better than doing it wrong.
*****
UPDATE: 3rd July 2014 – If you want to give your views on proposals to introduce tighter controls and safeguards on the use of personal health and care data do so by 8th August to Room 2N12. https://www.gov.uk/government/consultations/protecting-personal-health-and-care-data
Or respond online here> http://consultations.dh.gov.uk/data-sharing/protecting-health-and-care-information
[links 1-8 reference Part One]
[1] The NHS England Open House recording June 17th http://www.nhsengland-openhouse.public-i.tv/core/portal/NHSopenhouse
[2] IPSOS Mori poll conducted for the Joseph Rowntree Foundation: http://www.ipsos-mori.com/Assets/Docs/Polls/jrrt-privacy-topline-nhs-2014.pdf
[3] My post on uses of our records with commercial Data Brokers – https://jenpersson.com/flagship-care-data-2-commercial-practice/
[4] The Information Governance Review ‘Caldicott 2‘ https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/192572/2900774_InfoGovernance_accv2.pdf
[5] The Personal demographics Service at HSCIC (including name) http://systems.hscic.gov.uk/demographics/pds/contents
[6] The Data Linkage Service at HSCIC http://www.hscic.gov.uk/dles
[7] The Partridge review: http://www.hscic.gov.uk/datareview
[8] Summary Care Record use statistics https://www.whatdotheyknow.com/request/scr_care_settings_with_viewing_c#incoming-446569
[9] Minutes of the November Health & Adult Social Care Select Committee in Chichester http://www2.westsussex.gov.uk/ds/cttee/hasc/hasc141113ucmins.pdf
[10] The Quality of Nationally Submitted Health and Social Care Data, England – 2013, Second annual report, Experimental statistics – http://www.hscic.gov.uk/catalogue/PUB11530
[11] My post on commercial use of data with brokers
[12] Falsified hospital waiting times: The Telegraph http://www.telegraph.co.uk/health/healthnews/10590713/One-in-four-hospitals-records-false-waiting-times.html
***
Sales of 1984 have rocketed since the Snowden story broke in 2013: http://www.latimes.com/books/jacketcopy/la-et-jc-nsa-surveillance-puts-george-orwells-1984-on-bestseller-lists-20130611-story.html