On Friday 1st August the media reported the next giant leap in the genomics programme in England, suggesting the 100K Genomics Project news was akin to Kennedy launching the Space Race. [1] [from 2:46.30].
“The UK is set to become the world leader in ground-breaking genetic research into cancer and rare diseases, which will transform how diseases are diagnosed and treated, thanks to a package of investment worth more than £300 million.” [DH press release, August 1 2014. [2] ]
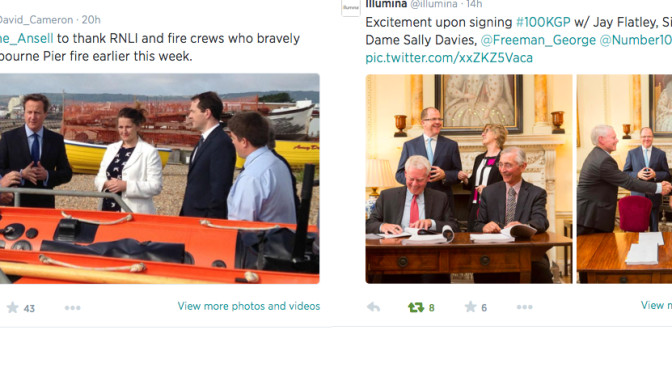
Whilst Mr. Cameron & George Osborne visited the arson-damaged Eastbourne Pier, the lifeboat staff and firemen who attended, back in Downing Street, representatives led by George Freeman MP signed the £300M investment package, the next step in the genomic investment plan, with American Jay Flatley, CEO of Illumina.
Mr. Cameron first announced this research drive shared with commercial pharmaceutical companies on 6th December 2011 and famously said ‘every willing patient should be a research patient'[3] (video) and they would consult to change the NHS Constitution to enable it:
“…with their medical details “opened up” to private healthcare firms, says David Cameron.”

This was the next step in the programme, hailed as an historic moment, a giant leap forward for genomics.
The photo call for the symbolic signing included Jay Flatley President, Chief Executive Officer and a member of the Board of Directors of Illumina, Inc, Sir John Chisholm Executive Chair of Genomics England & Chair of Nesta, together with Dame Sally Davies Chief Medical Officer and Mr. George Freeman [George 2] MP for mid-Norfolk, and the newly appointed Life Sciences Minister.
Fewer than twelve months before an election the Government has decided to commit commercially to a US based company, in a programme which Mr.Cameron himself said, has had controversy. That c-word is one the Conservatives will want to avoid in the coming election campaign.
This Channel 4 [4] film from almost 2 years ago, (December 2012) raises many questions as valid today as then. At that time, in contrast with today’s approach, the programme suggests that consent for research and data use would be assumed for all.
The inestimable Jon Snow asked then, why is the Business Department announcing this [the launch of the pilot programme, when focused then first in rare cancers]? The public may understand that commercial pharma, charities and the State work hand-in-glove (as Mr.Cameron’s 2011 vision stated), but as Jon Snow asks, not yet understand how this commercial venture will benefit the NHS long term as well as individual patients and the public as a whole? Is it concrete on benefits to patients vs benefits to UK plc?
So what was the key press message which came over?
The coverage of the week since August 1st, expounded the belief that through Genomics England Ltd we will do away with chemotherapy in the future. I believe this should be the source of a raging debate, but it passed by with little more than a few waves.
“We will look back in 20 years’ time and the blockbuster chemotherapy drugs that gave you all those nasty side effects will be a thing of the past,”said Jeremy Farrar Director of the Wellcome Trust, reported Sky. [5]
The original review given last summer to Genomics England including listing the rare diseases which may affect the 6% of the population, suggests one consideration, targeting those with very high likelihood of familial links and therefore success.[6] or Patients selected with a high probability of a single gene disorder. There are obviously great challenges in turnaround time for the genetic processing to be useful in clinical decision making. Considering whether or not it is timely or accurate enough to be of clinical benefit in acute cancer care clinical decision making will be vital. It is also what is being promised to patients who sign up, a faster, more efficient, improved offering on what is available already in the NHS genetic services today.
The interested population and profession would do well to get an independent medical update on the status of this, to understand it better if this is now established and its reliability, so what participants sign up for, is what they get on the tin:
“Results are provided for patients in a timely fashion (e.g. within 8 weeks) and with sufficient clinical accuracy (not yet established for WGS) [whole genome sequencing].” [page 3 of 8]
And what was the press result and public reaction to the news?
As one example, look at lunchtime on Friday August 1st, Radio 2 callers to the Jeremy Vine show. They included two undergoing chemo who felt they had to call in, to tell others, chemo is not always as bad as it sounds and make sure you don’t give up on it, refuse treatment or wait for this new genetic solution.
The impression was given, there is a new wonder solution within grasp on the horizon. This seemed to me rather reckless and unfairly manipulative on the ill and vulnerable to give them a blanket hope, that their cancer treatment may become so much better, soon. These are real people’s lives, not guinea pigs with which one can feel free to trial hypothesis and hype. If anyone now refuses chemo as a result of the Friday fantasy projections, their health may have been directly impacted. I would like to have heard a DH or Genomics England press manager speaking, not allowing such public free rein, to ensure it was factually accurate. But I’m guessing that Genomics England as an ALB is not really ready for press yet [their public engagement and education programme isn’t ready yet they confirmed when asked in July in an FOI], and the DH perhaps at arms length, thinks, it’s not their responsibility and outside their remit. Stuck in the middle, we have the commissioning body, NHS England.
How might this involve all of us, our NHS and cross into care.data?
In most recent memory, NHS England tried and so far failed in February 2014, to engage the public and clinicians in the extraction of our GP stored health records, in the care.data initiative. Care.data languishes in some sort of unknown black hole at the moment, with little public engagement and pilots promised ‘for autumn’. Both programmes are run under the auspices of Mr. Kelsey at NHS England Patients and Information Department, and arms length from the Department of Health. Last summer, Tim Kelsey and Sir Bruce Keogh presented a paper to the Board on Genomics and its interaction with NHS patient records. [7]
Given that the Genomics paper indicated that care.data and NHS held patient records were of paramount importance to NHS England I would like to have seen more transparency over this, including informed public and parliamentary debate:
“Issues of data ownership and transparency are of paramount importance to NHS England as set out in the Mandate and given the hugely positive developments in Care.Data. Geraint Lewis is leading this work, and has begun work to consider how the sequencing data might be held, connected to patient records and subsequently be exploited. It will also look at the connections between this work and the establishment of care data in the NHS. The NHS England data and informatics team will retain oversight of the informatics and data work and discussions continue on how it can best inform and support the implementation of business plan of Genomics England Limited.”
NHS England Board paper, July 2013 [7]
There has been almost no public statement from NHS England on genomics and our data management in the same discussion, until now. George Freeman MP [2] said on BBC Radio 4 (Starting from 2:46.30 in interview with Sarah Montague:
“It’s absolutely not the care.data initiative discussed earlier in the year. This is 100K patients, all volunteering and all providing their consent. It’s completely anonymised data in the data set, the only person who would be able to come back to the patient and make a link with the genomics and the diagnosis, is their doctor. We’re creating a database so that NHS researchers and industry researchers, can look at the broad patterns. 90% of patients with that variation, get that disease, this drug works in 50% of patients…It’s completely anonymised, there is no basis on which you could make the link. The only person who can make the link is the NHS clinician.”
Whilst this is NOT the same initiative, it intends to use some of the same data for those people who actively consent to participate in the 100K Genome Project.
The data will be extracted from care.data [which ‘assumes consent’ or requires active opt OUT, depending how you view it] to include longitudinal, phenotype data across a person’s lifetime. I spoke to the Genomics England media team last autumn, 2013, which confirmed this intent at that time.
The trouble is for Mr. Freeman [2] and these statements, that the public knows ‘anonymous’ in care.data turned out to not be anonymous at all. ICO and HSCIC [8] are still working this out. [HSCIC has just published its first review of pseudonymisation review 9] It was discovered that far from being released only to clinicians and researchers, our hospital data has been shared with all sort of unexpected third parties, without consent. [see the Partridge Review]. This surprised and shocked many, to public outcry and the resultant loss of trust [15] in the programme has yet to be rebuilt. So some listeners may well and understandably have had concerns that their data may be used for purposes to which they have not agreed.
Some say that genetic data by its very nature, despite stripping data identifiers, cannot be non-identifying, or stay that way:[16]
“It only takes one male,” said Yaniv Erlich, a Whitehead fellow, who led the research team. “With one male, we can find even distant relatives.” [Jan 2013]
“If they choose to share that’s a very admirable thing because by sharing freely, progress for everyone is accelerated, and if someone is not comfortable we should respect that too and find ways for them to still participate in research,” he said.
What are the next steps – or should we expect, one giant leap?
As regards care.data from all, it is I believe reasonable, that we should we ask: how we should expect our care.data to be used, and trust for what restricted purposes it will be extracted and stored for the future? What mechanisms will separate consent for care.data commissioning from this kind of research? How will citizens trust this data sharing now as the Department for Patients and transformation care.data proposals seem still open ended in scope in particular for social care [17], and alongside other ever widening government data sharing? [18] How will the public know where the future boundaries of care.data scope creep lie?
If anything has been learned from care.data to date it must be this: We should continue to ask for more public involvement in policy and planning, not just the post-event PR if the state wishes to ensure success and prevent surprises. What happens next for this data programme, and for our national programme of genomics, 100K?
******
[1] “It’s a hugely ambitious project, it’s on a par with the space race how Kennedy launched 40 years ago.” [from 2:46.30 BBC Radio 4 Int. Sarah Montague w/ George Freeman]
[2] Downing Street Press Release 1st August – genomics https://www.gov.uk/government/news/human-genome-uk-to-become-world-numb
[3] 6th December “Transcript of a speech given by Prime Minister at the FT Global Pharmaceutical and Biotechnology Conference” [https://www.gov.uk/government/speeches/pm-speech-on-life-sciences-and-opening-up-the-nhs]
[4] 10th December 2012 DNA Database concerns Channel 4 http://www.channel4.com/news/dna-cancer-database-plan-prompts-major-concerns
[5] Wellcome Trust- comment by Jeremy Farrar http://news.sky.com/story/1311189/pm-hails-300m-project-to-unlock-power-of-dna
[6] Strategic Priorities in Rare Diseases June 2013 http://www.genomicsengland.co.uk/wp-content/uploads/2013/06/GenomicsEngland_ScienceWorkingGroup_App2rarediseases.pdf
[7] NHS England Board paper presentation July 2013 http://www.england.nhs.uk/wp-content/uploads/2013/07/180713-item16.pdf
[8] ICO and HSCIC on anonymous and pseudonymous data in Computing Magazine http://www.computing.co.uk/ctg/news/2337679/ico-says-anonymous-data-not-covered-by-data-protection-act-until-its-de-anonymised
[9] HSCIC Pseudonymisation Review August 2014 http://www.hscic.gov.uk/article/4896/Data-pseudonymisation-review
[10] November 2013 ISCG – political pressure on genomics schedule http://www.england.nhs.uk/iscg/wp-content/uploads/sites/4/2014/01/ISCG-Paper-Ref-ISCG-009-001-ISCG-Meeting-Minutes-and-Actions-26-November-2013-v1.1.pdf
[11] Wellcome Trust August 1st 2014 The Genetic Building Blocks of Future Healthcare
[12] Fenyan – For successful technology reality must take precedence over PR https://jenpersson.com/successful-technology-reality-precedence-public-relations/
[13] Next Steps in the Sequence – the implications for whole genome sequencing in the UK – PHG Foundation, funded by the PHG Foundation, with additional financial support from Illumina. The second expert workshop for the project was supported by the University of Cambridge Centre for Science and Policy (CSaP) and the Wellcome Trust http://www.phgfoundation.org/file/10363
[14] Anti-elderly drugs proposals rejected by NICE: Channel 4 http://www.channel4.com/news/nice-assessment-elderly-health-drugs-rejected-contribution
[15] The Royal Statistical Society identifies a Trust Deficit
*****
For avoidance of confusion [especially for foreign readership and considering one position is so new], there are two different Ministers mentioned here, both called George:
One. George Osborne [George 1] MP for Tatton, Cheshire and the Chancellor
Two. George Freeman [George 2] MP – The UK’s first-ever Minister for Life Sciences, appointed to this role July 15th 2014 [https://www.gov.uk/government/ministers/parliamentary-under-secretary-of-state–42]
*****