Enabling public trust in data sharing is not about ‘communicating benefits’. For those interested in nitty gritty, some practical suggestions for progress in Building Public Trust in data sharing follows on from my summary after the NIB Bristol event 24/7/15.
Trust is an important if invisible currency used in the two-way transactions between an organisation and people.
So far, there have been many interactions and listening events but much of what professionals and the public called for, remains undone and public trust in the programme remains unchanged since 2014.
If you accept that it is not public trust that needs built, but the tangible trusthworthiness of an organisation, then you should also ask what needs done by the organisation to make that demonstrable change?
What’s today’s position on Public Trust of data storage and use
Trust in the data sharing process is layered and dependent on a number of factors. Mostly [based on polls and public event feedback from 2014] “who will access my data and what will they use it for?”
I’m going to look more closely below at planned purposes: research and commissioning.
It’s also important to remember that trust is not homogeneous. Trust is nuanced even within the single relationship between one individual and another. Trust, like consent, is stratified – you may trust the Post Office to deliver a letter or postcard, but sign up to recorded delivery for something valuable.
So for example when it comes to secondary uses data sharing, I might trust HSCIC with storing and using my health records for anonymous statistics, for analysis of immunisation and illness patterns for example. But as long as they continue to share with the Home Office, police or other loosely defined third parties [5], do I want them to have fully identifiable data at all?
Those bodies have their own public trust issues at an all time low.
Mixing the legitimate users of health data with these Back Office punitive uses will invite some people’s opt out who would otherwise not. Some of the very groups who need the most health and social care understanding, research and care, will be the very groups who opt out if there is a possibility of police and Home Office access by the back door. Telling traveller communities what benefits care.data will bring them is wasted effort when they see NHS health data is a police accessible register. I know. I’ve talked to some about it.
That position on data storage and use should be reconsidered if NHS England is serious that this is about health and for the benefit of individuals and communities’ well being.
What has HSCIC changed to demonstrate that it is trustworthy?
A new physical secure setting is being built that will enable researchers to view research data but not take raw data away.
That is something they can control, and have changed, and it demonstrates they take the public seriously and we reciprocate.
That is great – demonstrable change by the organisation, inviting change in the public.
That’s practical, so what can be done on policy by NHS England/DH?
What else should be done to demonstrate policy is trustworthy?
Act on what the public and professionals asked for in 2014. [8]
Right now it feels as though in public communications that the only kind of relationship that is wanted on the part of the leadership is a one night stand.
It’s all about what the programme wants. Minimise the objections, get the data, and sneak out. Even when its leaders talk about some sort of ongoing consent model, the focus is still about ‘how to enable sharing data.’
This focus is the wrong one. If you want to encourage people to share they need to know why, what’s in it for them, and why do you want it? What collecting the data is about is still important to explain and specifically, each time the scope changes if you are doing it fairly.
Remember. Data-sharing is not vital to future-proof the NHS. Using knowledge wisely is.
What is the policy for the future of primary care research?
The CPRD already enables primary care GP data to be linked with secondary data for research. In fact it already links more items from GP held data than current are.data plans to extract. So what benefit will care.data offer to research that is not already available today?
Simply having ever more data, stored in more places will not make us wiser. Before it’s collected repeatedly, it is right to question why.
What do we have collected already? How is it used? Where are the gaps in what we want to achieve through the knowledge we could gain. It’s NOT simply about filling in what gaps exist in what data we could gather. Understand the purposes and what will be gained to see if it’s worth the efforts. Prioritise. Collect it all, is not a solution.
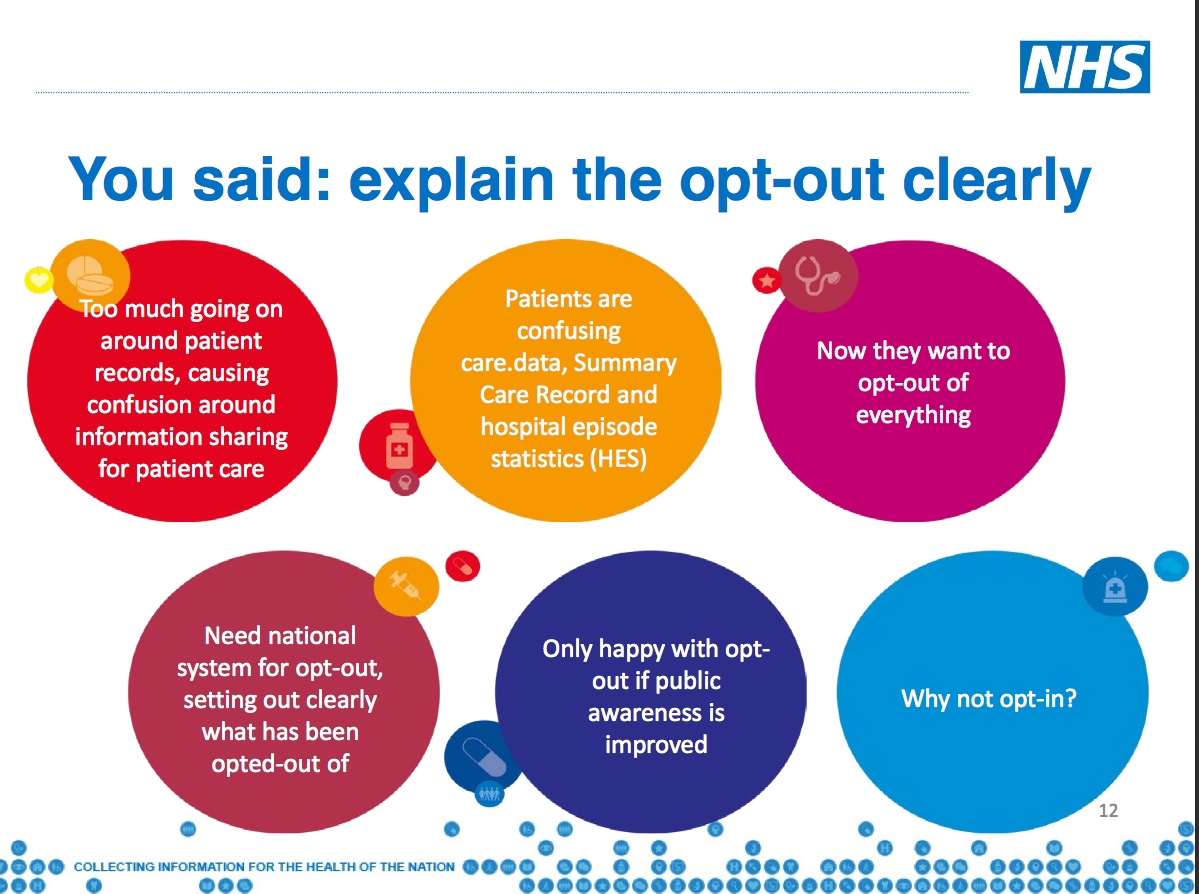
I had thought that the types of data to be collected in care.data were clear, and how it differs from direct care was clear. But the Bristol NIB meeting demonstrated a wide range of understanding in NHS and CCG staff, Local Authority staff, IT staff, IG professionals, data providers and other third parties. Data for secondary purposes are not to be conflated with direct care.
But that’s not what care.data sharing is about. So where to start with public trust, asked the NIB Bristol #health2020 meeting?
Do you ignore the starting point or tailor your approach to it?
“The NHS is at a crossroads and needs to change and improve as it moves forward. That was the message from NHS England’s Chief Executive Simon Stevens as a Five Year Forward View for the NHS was launched.” [1] [NHS England, Oct 2014]
As the public is told over and over again that change is vital to the health of a sustainable NHS, a parallel public debate rages, whether the policy-making organisations behind the NHS – the commissioning body NHS England, the Department of Health and Cabinet Office – are serious about the survival of universal health and care provision, and about supporting its clinicians.
It is against this backdrop, and under the premise that obtaining patient data for centralised secondary uses is do or die for the NHS, that the NIB #health2020 has set out [2] work stream 4: “Build and sustain public trust: Deliver roadmap to consent based information sharing and assurance of safeguards”
“Without the care.data programme, the health service will not have a future, said Tim Kelsey, national director for patients and information, NHS England.” [3]
Polls say [A] nearly all institutions suffer from a ‘trust in data deficit’. Trust in them to use data appropriately, is lower than trust in the organisation generally.
Public trust in what the Prime Minister says on health is low.
Trust in the Secretary of State for Health is possibly at an all time low, with: “a bitter divide, a growing rift between the Secretary of State for Health and the medical profession.” [New Statesman, July 2015]
This matters. care.data needs the support of professionals and public.
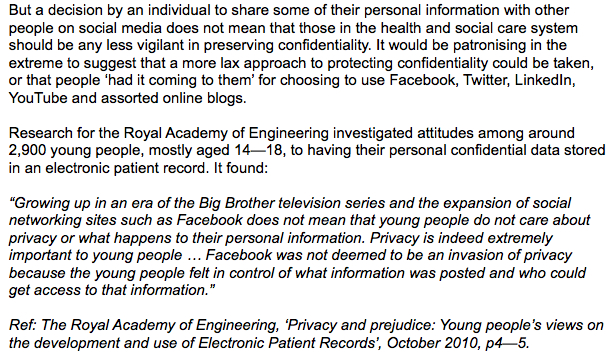
ADRN research showed multiple contributing factors: “Participants were also worried about personal data being leaked, lost, shared or sold by government departments to third parties, particularly commercial companies. Low trust in government more generally seemed to be driving these views.” [Dialogue on data]
It was interesting to see all the same issues as reflected by the public in care.data listening events, asked from the opposite perspective from data users.
But it was frustrating to sit ay the Bristol NIB #health2020 event and discuss questions around the same issues on data sharing already discussed at care.data events through the last 18 months.
Nothing substantial has changed other then HSCIC’s physical security for data storage.
It is frustrating knowing that these change and communications issues will keep coming back again and again if not addressed.
Personally, I’m starting to lose trust there is any real intention for change, if senior leadership is unwilling to address this properly and change themselves.
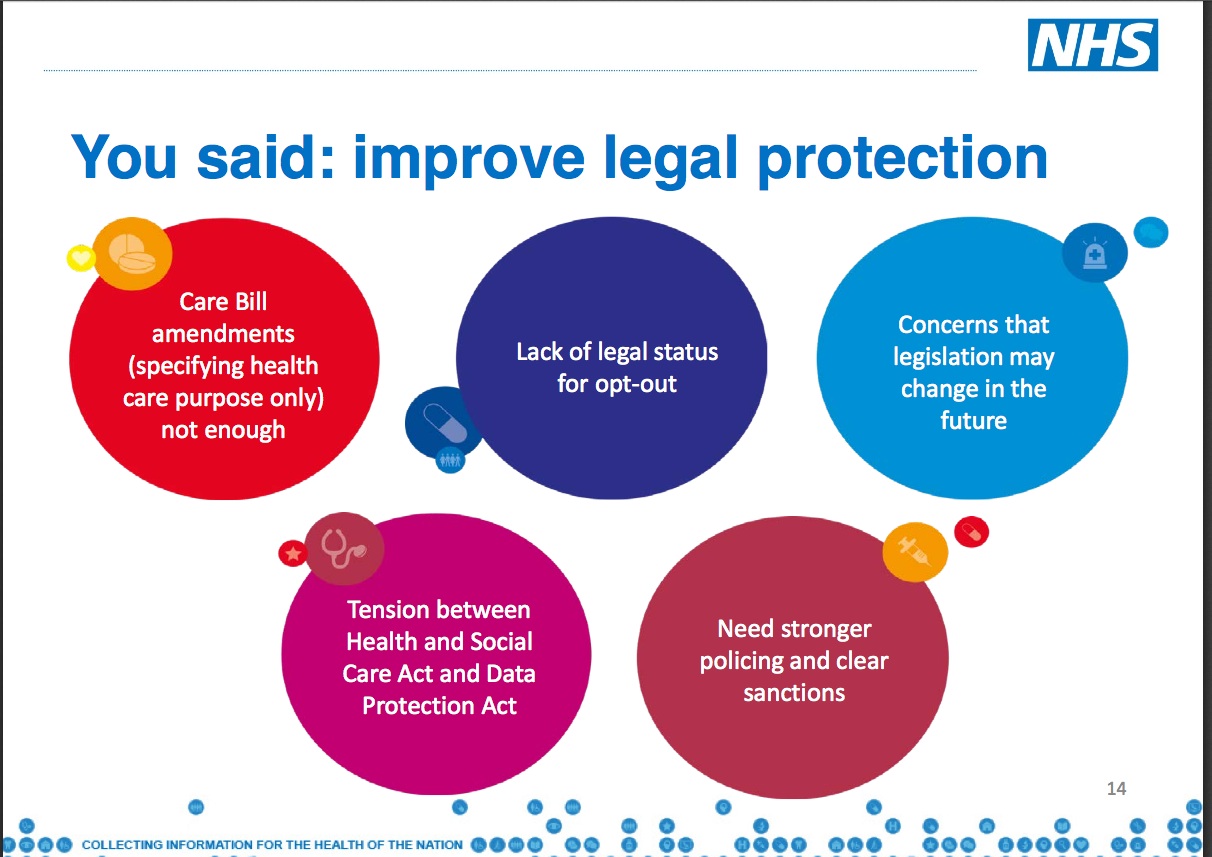
To see a change in Public Trust do what the public asked to see change: On Choice
At every care.data meeting I attended in 2014, people asked for choice.
They asked for boundaries between the purposes of data uses, real choice.
Willingness for their information to be used by academic researchers in the public interest does not equate to being willing for it to be used by a pharmaceutical company for their own market research and profit.
The public understand these separations well. To say they do not, underestimates people and does not reflect public feeling. Anyone attending 2014 care.data events, has heard many people discuss this. They want a granular consent model.
This would offer a red line between how data are used for what purposes.
Of the data-sharing organisations today some are trusted and others are not. Offering a granular consent approach would offer a choice of a red line between who gets access to data.
This choice of selective use, would encourage fewer people to opt out from all purposes, allowing more data to be available for research for example.
To see a change in Public Trust do what the public asked to see: Explain your purposes more robustly
Primarily this data is to be used and kept indefinitely for commissioning purposes. Research wasn’t included as purposes for care.data gathering in the planned specifications for well over a year. [After research outcry]
Yet specific to commissioning, the Caldicott recommendations [3] were very clear; commissioning purposes were insufficient and illegal grounds for sharing fully identifiable data which was opposed by NHS England’s Commissioning Board:
“The NHS Commissioning Board suggested that the use of personal confidential data for commissioning purposes would be legitimate because it would form part of a ‘consent deal’ between the NHS and service users. The Review Panel does not support such a proposition. There is no evidence that the public is more likely to trust commissioners to handle personal confidential data than other groups of professionals who have learned how to work within the existing law.”
NHS England seems unwilling to change this position, despite the professionals bodies and the public’s opposition to sharing fully identifiable data for commissioning purposes [care.data listening events 2014]. Is it any wonder that they keep hitting the same barrier? More people don’t want that to happen than you do. Something’s gotta give.
Ref the GPES Customer Requirements specification from March 2013 v2.1 which states on page 11: “…for commissioning purposes, it is important to understand activity undertaken (or not undertaken) in all care settings. The “delta load” approach (by which only new events are uploaded) requires such data to be retained, to enable subsequent linkage.”
The public has asked for red lines to differentiate between the purposes of data uses. NHS England and the Department of Health policy seems unwilling to do so. Why?
To see a change in Public Trust do what the public asked to see: Red lines on policy of commercial use – and its impact on opt out
The public has asked for red lines outlawing commercial exploitation of their data. Though it was said it was changed, in practice it is hard to see. Department of Health policy seems unwilling to be clear, because the Care Act 2012 purposes remained loose. Why?
As second best, the public has asked for choice not to have their data used at all for secondary purposes and were offered an opt out.
NHS England leaflet and the Department of Health, Secretary of State publicly promised this but has been unable to implement it and to date has made no public announcement on when it will be respected. Why?
Trust does not exist in a vacuum. What you say and what you actually do, matter. Policy and practice are co-dependent. Public trust depends on your organisations being trustworthy.
Creating public trust is not the government, the DH or NIB’s task ahead. They must instead focus on improving their own competency, honesty and reliability and through those, they will demonstrate that they can be trusted.
That the secondary purposes opt out has not been respected does not demonstrate those qualities.
“Trust is not about the public. Public trust is about the organisation being trustworthy.”
How will they do that?
Let the DH/NHS England and organisations in policy and practice address what they themselves will stop and start doing to bring about change in their own actions and behaviours.
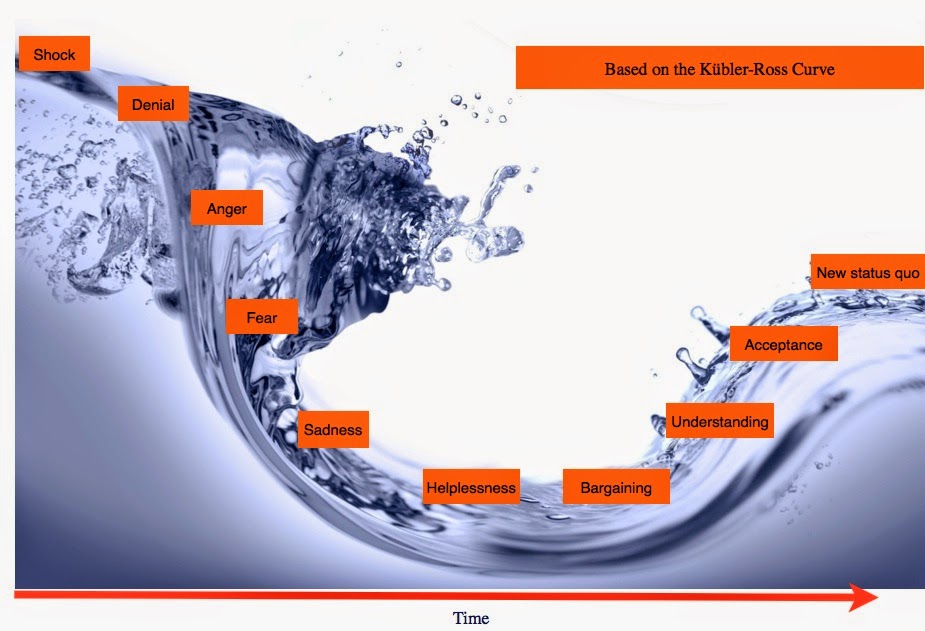
Communications change request: Start by addressing the current position NOT what the change will bring. You must move people along the curve , not dump them with a fait accomplice and wonder why the reaction is so dire.
Vital for this is the current opt out; what was promised and what was done.
The secondary uses opt out must be implemented with urgency.
To see a change in Public Trust you need to take action. the Programme needs to do what the public asked to see change: on granular consent, on commercial use and defined purposes.
And to gather suggested actions, start asking the right questions.
Not ‘how do we rebuild public trust?’ but “how can we demonstrate that we are trustworthy to the public?”
1. How can a [data-sharing] org demonstrate it is trustworthy?
2. Identify: why people feel confident their trust is well placed?
3. Why do clinical professionals feel confident in any org?
4. What would harm the organisational-trust-chain in future?
5. How will the org-trust-chain be positively maintained in future?
6. What opportunities will be missed if that does not happen?
(identify value)
Yes the concepts are close, but how it is worded defines what is done.
These apparent small differences make all the difference in how people provide you ideas, how you harness them into real change and improvement.
Only then can you start understanding why “communicating the benefits” has not worked and how it should affect future communications materials.
From this you will find it much easier to target actual tasks, and short and long term do-able solutions than an open discussion will deliver. Doing should include thinking/attitudes as well as actions.
This will lead to communications messages that are concrete not wooly. More about that in the next posts.
####
To follow, for those interested in nitty gritty, some practical suggestions for progress in Building Public Trust in data sharing:
Part one: A seven step top line summary – What I’d like to see change addressing public trust in health data sharing for secondary purposes.
This is Part two: a New Approach is needed to understanding Public Trust For those interested in a detailed approach on Trust. What Practical and Policy steps influence trust. On Reserach and Commissioning. Trust is not homogeneous. Trust is nuanced even within the single relationship between one individual and another. It doesn’t exist in a vacuum.
Part three: Know where you’re starting from. What behaviours influence trust and how can we begin to see them demonstrated. Mr.Kelsey discusses consent and opt out. Fixing what has already been communicated is vital before new communications get rolled out. Vital to tailor the content of public communications, for public trust and credibility the programme must be clear what is missing and what needs filled in. #Health2020 Bristol NIB meeting.
Part four: “Communicate the Benefits” won’t work – How Communications influence trust. For those interested in more in-depth reasons, I outline in part two why the communications approach is not working, why the focus on ‘benefits’ is wrong, and fixes.
Part five: Future solutions – why a new approach may work better for future trust – not to attempt to rebuild trust where there is now none, but strengthen what is already trusted and fix today’s flawed behaviours; honesty and reliability, that are vital to future proofing public trust.
####
References:
[1] NHS England October 2014 http://www.england.nhs.uk/2014/10/23/nhs-leaders-vision/
[2] Workstream 4: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/442829/Work_Stream_4.pdf
[3] Caldicott Review 2: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/192572/2900774_InfoGovernance_accv2.pdf
[4] Missing Programme Board documents: 2015 and June-October 2014
[5] HSCIC Data release register
[6] Telegraph article on Type 2 opt out http://www.telegraph.co.uk/news/health/news/11655777/Nearly-1million-patients-could-be-having-confidential-data-shared-against-their-wishes.html
[7] Why Wanting a Better Care.Data is not Luddite: http://davidg-flatout.blogspot.co.uk/2014/04/why-wanting-better-caredata-is-not.html
[8] Talking to the public about using their data is crucial- David Walker, StatsLife http://www.statslife.org.uk/opinion/1316-talking-to-the-public-about-using-their-data-is-crucial
[9] Dame Fiona Caldicott appointed in new role as National Data Guardian
[10] Without care.data health service has no future says director http://www.computerweekly.com/news/2240216402/Without-Caredata-we-wont-have-a-health-service-for-much-longer-says-NHS
[11] Coin Street, care.data advisory meeting, September 6th 2014: https://storify.com/ruth_beattie/care-data-advisory-group-open-meeting-6th-septembe
[12] Public questions unanswered: https://jenpersson.com/pathfinder/

![Building Public Trust in care.data datasharing [3]: three steps to begin to build trust](https://jenpersson.com/wp-content/uploads/2015/06/optout_ppt-672x372.jpg)
![Building Public Trust [2]: a detailed approach to understanding Public Trust in data sharing](https://jenpersson.com/wp-content/uploads/2015/03/Trust-e1426443553441-672x372.jpg)
![Building Public Trust in care.data sharing [1]: Seven step summary to a new approach](https://jenpersson.com/wp-content/uploads/2015/07/edison1-672x372.jpg)