
“O my Luve’s like a red, red rose, that’s newly sprung in June: O my Luve’s like the melodie, That’s sweetly play’d in tune.
As fair art thou, my bonnie lass, so deep in luve am I; And I will luve thee still, my dear, Till a’ the seas gang dry. […]”
Robert Burns, 1759-1796 [aged 37]
Friends and I hold a Burns Supper every year. What began as a one off, was repeated in a different home, with the same dozen guests a year later. So a tradition was born to celebrate the life and works of Scotland’s most famous export.
“His national pride, fierce egalitarianism, and quick wit have become synonymous with the Scottish character itself.” Robert Burns Birthplace Museum, Dumfries
Burns was famous for his belief in equality, and his poem “Is There for Honest Poverty“, commonly known as “A Man’s a Man for A’ That” of 1795 declared a stance in society, seen today as the rise of a liberalism, which is declared the world over today still. It is often used by the Freemasons as Burns was at the time of his death. It is the fierce pride in humanity of man that infuses Burns’ work and which has transcended time. His love poetry, and rural recordings, being ‘ahead of his time’ made him memorable. But I feel it was his awareness and discussion of identity and social-economic politics which still inspires and what makes his work contemporary.
The Burns Night Declaration
Perhaps it is some of that inspiration that Westminster hoped to capture by naming the latest political deal, granting Scotland more rights which Mr. Brown pledged this week, “The Burns Night Declaration.”
Scots have been promised “modern home rule within the United Kingdom” on a breakneck timetable on Monday if they rejected independence next week.”
From a personal perspective
I think there is a real chance of a yes vote. If Scotland were to vote for independence next week, I will celebrate the freedom, with a divided allegiance. The Scottish ‘heart’ in me will stir with a rallying cry and remember my ancestors who died on the fields of Bannockburn. My English ‘head’ will be disappointed, as I worry for the country downsizing to the size of Denmark will be a shock, and not fully thought out change, without a leader who can bring the whole country together. I foresee a future in which the Celts are ruled still rather than greater independence for Scotland, with more dominant powers from Brussels instead of London as they seek strength and support as they once did with France in the Auld Alliance, rallying against English oppression. Should there be a yes vote, I will be dispirited, whilst clinging to optimism of change.
I have concerns about the economy, research investment, about its potential effect on the NHS and education provision, arguably better for the people than in England today. But in the end, my concerns don’t count, it is for the Scots in Scotland to decide.
As a Scot living in England, I have no vote. For my part, that is quite alright. For another Scot I know who fully intends moving back ‘up North’ and going ‘home’ in some years time, she is devastated at the thought of Scotland going solo, and that she has no say. Her sister still in Scotland, who can vote, was among those who received a letter in which she felt that it hinted that her employer, the Job Centre, may be put in jeopardy from a yes vote. [She may be right if DWP would need to be significantly ‘disentangled’ according to this report.] She’s considering voting yes anyway. Why?
Because at local level she thinks their jobs are in jeopardy of potential outsourcing regardless of the vote.
Because she’s lived through years of ‘better together’ and has seen only a decline in standards of living and no one has seemed to really seek to change that. She may not realise, Scotland is not alone in this, but with little elected power in Westminster, they may see independence as their only hope of change.
Because she feels democratically disempowered. No matter who she votes for today, it still results in not getting who they want in charge of government, and no way to oust them if a few areas of England vote that person in. The overall budget control for Scottish spending comes from Westminster. And lastly, in terms of governance, whilst necessary, adding experience and a system of ‘check and balance’ on legislation, the unelected House of Lords sits only in London and can appear accountable to no one, never mind the Scots.
How may politics be affected by the outcome?
I hear many people have had enough of imposed rule as they see it and disconnected leaders. One may think through devolution, more powers for Holyrood would have satisfied the desire for autonomy, but in fact people are fed up with the rhetoric of the political rule from both Westminster and Edinburgh.
Many dislike the leadership choices on offer [latest FullFact poll stats here Sept 11th]. Women in particular appear to consider this important in their decision. Should the yes vote win, it will not necessarily be a win for Mr. Salmond, but a win for independence.
Key is, what will that independence really look like? It will be interesting to see. Would it be what Mr. Salmond expects? What scenarios have been thought out [1], debated, and what may have been missed?
The red rose of Labour has become faded in Scotland. This has and will continue to have an impact on future General Elections. I believe however, it must be encouraged to continue to grow, come back and actively thrive in Scotland regardless of this vote outcome. All mainstream parties would do well consider this, above party politics. There is a risk that the disenchantment with mainstream politics will give rise to more extreme factions. A sense of identity is a good thing, but at its extreme can be twisted into a damaging minority view of nationalism which is based on one group view over another, the real-world diversity of a nation excluded. Should mainstream parties leave a vacuum in the garden of Scottish politics, others will be quick to fill it, and it is often ugly weeds which take root fastest.
How has the People’s involvement in politics been affected?
Perhaps the best thing about this campaign has been an awakening. An awakening of people’s role in the democratic process, exemplified by the planned march on voting day in one area of Glasgow. Where low turnout is typical organisers aim to stir people and carry them with them, to the polls, [which may or may not be legal electoral practice]. There has been an unprecedented number of electoral registrations. But also an awakening of the big parties that your action and inaction matters. It has been forgotten in recent apathy. This awakening will not be restricted to Scotland, and politicians across Europe should learn from these experiences quickly, as calls for independence in other places are bound to come.
The Scots are inspirational to many. Whilst fiction, the spirited speech of William Wallace in Braveheart calls to the basic instinct in us all, for freedom. We Scots have a strong sense of history as part of our identity. Entwined in that is the relationship between the wealthy landed Scots and the English nobility, and the complex succession of the throne and in-fighting of Scots lairds. Who sided with whom, when and how trust was won and lost became glorified legend in Rob Roy and Braveheart, but it’s not all based on fiction, but historical fact.
What has been perhaps unfairly represented by some media headlines and survey statistics, is the image of how “the English” feel about “the Scots” and how the two countries would be after a yes vote. One survey showed well over 66% in favour of the Union, but the survey chose to represent a subjective statement on currency as its headline, for example. Poll upon poll state conflicting measures as ‘fact’. It is hard to separate fact from feeling in an emotive debate.
A Troubled Relationship
If you are not Scottish, you may or may not be familiar with the Scot’s spirit of the everyday, not celebrities nor stereotypes. If you have time, listen to this speech, a Burns night reply from the lassies. It gives the ladies a chance to ‘get their neb in’. (4.28) It’s meant to be tongue in cheek and irreverent, and not to take the subject too seriously, and this hits the spot. But mainly because it hints at something of what matters to Scots in a speech about Burns. In particular it’s worth considering this one snippet. With humour she tells us what matters above politics and above class, is relationships and communication. It is the relationship and communication that has broken down between Westminster and the people in Scotland which may be the Union’s downfall. The Scottish People feeling neglected, had stopped talking to Westminster a long time ago, and Westminster didn’t notice.
Robert Burns understood People
Burns was a poet, a man of love and passion. A man of the heart. A man popular with women, a philanderer, yet perhaps one of the first feminists? Not a warrior, not a career politician, he was a man for the people. He recognised women’s rights above and amongst politics, and spoke up on our behalf:
“While Europe’s eye is fix’d on mighty things,
The fate of empires and the fall of kings;
While quacks of State must each produce his plan,
And even children lisp the Rights of Man;
Amid this mighty fuss just let me mention,
The Rights of Woman merit some attention.”
Visiting politicians would do well to appeal to the rights of women as Burns did. I believe that it is not a romantic notion of freedom, which will lead to a majority of the yes vote. It is another practical aspect of life exemplified in Burns’s poetry which matters to people today, and how we live. It can affect all, but disproportionally affects women, it is poverty:
These last minute efforts of visiting politicians may or may not be planned in the campaign. But as Burns said,
“The best laid schemes o’ mice an’ men gang aft agley.”
The politicians may visit all they like, for a day or a week, better late than never. It will not make or break the majority of voters, voting with their head based on practical matters, but it may influence the ‘don’t noes’ the ‘vote for freedom’ who vote only with the heart at the last minute, and influence enough to swing the outcome. The majority of people will decide based not on last ditch efforts and promises, but on how they want to live, and what kind of society they want to see. Will speeches and promises made in a week, override experiences of many years? Or will they swing an influential minority?
The question is how convinced will voters be of the need for a complete break from the United Kingdom and true independence with its associated risk, versus the offering in the Burns Night Declaration? How much will heart rule the head or vice versa?
Whichever way the vote may go, how will mainstream political parties react and cultivate the long term relationship between Scotland and England? There will be a period between the vote and enactment. How will uncertainty be handled in that interim? How will the yes and no factions keep talking to one another, and grow as one nation, whether in a united, devolved or separate states?
O my Luve’s like a red, red rose
Scotland whichever path you choose to take, I will follow your decision closely. Whatever happens next week, some will be broken hearted. I hope I won’t be among them. And I hope that for those who are disappointed with the outcome, we will all be kind, encouraging and not seek to blame, as we go about restoring our trust, our relationships and grow together in a positive, new direction. Society cannot afford a political vacuum which will provide space for the weeds of extremism to grow between us.
Wherever we are born, it is not unexpected to continue to have positive feelings for that country, as our birthplace. I may have left over thirty years ago, but my heart is still in the Highlands. I still love Scotland and hope she still loves us enough to stay together.
But I’ll understand if not.
“But to see her was to love her,
Love but her, and love forever.
Had we never lou’d sae kindly,
Had we never lou’d sae blindly,
Never met – or never parted –
We had ne’er been broken hearted”
Robert Burns, 1759-1796
***
[1] Governing after the Referendum – by the Institute for Government http://www.instituteforgovernment.org.uk/sites/default/files/publications/Scenarios%20paper%20-%20final%20APJR.pdf
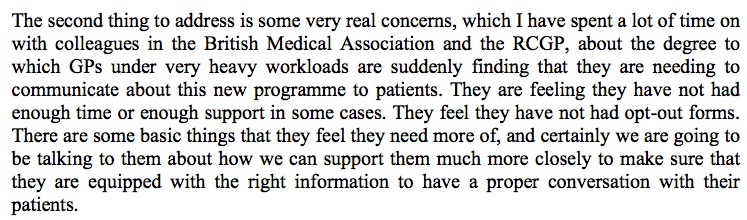
![Care.data – my six month pause, anniversary round up [Part 1]](https://jenpersson.com/wp-content/uploads/2014/08/gps_controller-672x245.jpg)
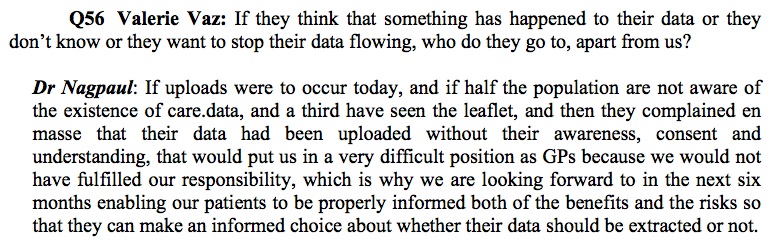
![Care.data – my six month pause, anniversary round up [Part 2]](https://jenpersson.com/wp-content/uploads/2014/08/first-672x216.jpg)


![Launching genomics, lifeboats, & care.data [part 2]](https://jenpersson.com/wp-content/uploads/2014/08/rosetta_image-672x372.jpg)

![care.data should be like playing Chopin – or will it be all the right notes, but in the wrong order? [Part one]](https://jenpersson.com/wp-content/uploads/2014/07/chopin-664x372.jpg)